
Most of the compounds discussed below are not FDA-approved, several are prohibited in competitive sport, and the human evidence for muscle recovery and strength is limited. Used responsibly, that means a prescription and a licensed pharmacy, not a vial ordered off a research-chemical site.
There’s a specific confusion running through fitness forums and supplement threads right now, and it goes something like this: growth hormone repairs tissue, so anything that raises growth hormone should speed recovery, cut soreness, and protect muscle during hard training blocks. It’s a tidy story. It’s also, on closer inspection of the actual clinical literature, mostly untested where it matters most.
This piece sets out to untangle that confusion for anyone who has read a caption about “overnight repair” and wondered whether it holds up. It walks through what the studies actually measured (not what the marketing implies they measured), and then through the more practical question the hype conveniently skips: if someone decides to try one of these anyway, who should be standing between them and the syringe.
The pitch, stated as its believers state it
The recovery-and-strength corner of peptide culture leans on a few familiar names. MK-677 gets pitched for “overnight repair.” GHRP-6 is framed as a recovery-and-appetite combo. CJC-1295 is marketed as “sustained repair hormone.” Follistatin 344 gets the boldest claim of all, that it doesn’t just build muscle but protects and rebuilds it by releasing the natural brake the body places on muscle tissue, myostatin.
Each of these claims rests on a real mechanism. That’s precisely what makes them persuasive and also what makes them slippery. These peptides genuinely do interact with the growth hormone and IGF-1 system. The open question, the one worth actually reading the primary literature to answer, is whether that biochemical activity turns into the human outcomes people are told to expect: less soreness, faster bounce-back, more strength. That’s a different claim than “raises a hormone,” and it needs its own evidence.
The clarification: what the studies actually measured
Here is the gap, compound by compound, between the mechanism and the promised outcome.
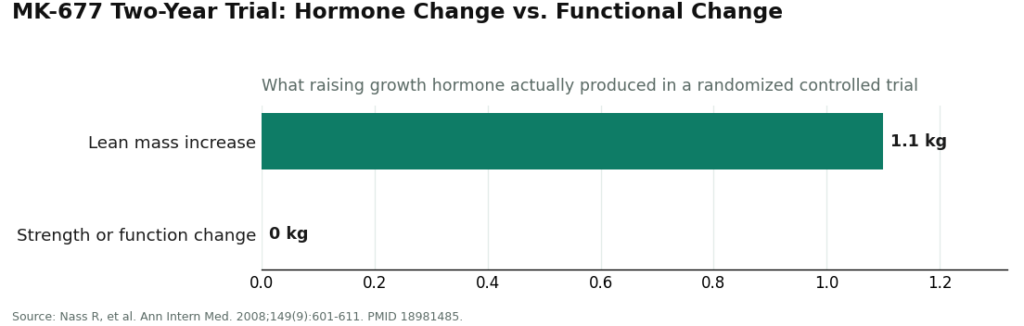
MK-677 (ibutamoren) has the most substantial human data of the group, which is exactly why its result matters so much. In a two-year randomized controlled trial, MK-677 raised growth hormone and IGF-1 and increased lean mass by about 1.1 kg. But the increase “did not result in changes in strength or function” [1]. This is the compound with the longest, most rigorous human trial in the category, and it’s the one that most directly tested the recovery crowd’s core assumption. The hormone went up. Lean mass went up slightly. Strength and function did not follow.
CJC-1295 carries the “sustained repair hormone” reputation, and the underlying pharmacology really is notable: in healthy adults, it raised growth hormone and IGF-1 for days after a single dose [2]. What that study did not do is measure recovery, soreness, strength, or function. It confirms the input the recovery pitch assumes exists. It says nothing about the output the pitch actually promises.
GHRP-6 is well established in the pharmacology of growth hormone release. Combined with GHRH, it produces a bigger growth hormone response than either compound alone in controlled human research [3]. Again, that’s a hormone-release finding, not a recovery finding. There’s no solid human evidence tying it to faster healing or measurable strength gains in healthy adults.
Follistatin 344 is where the hype and the evidence diverge most sharply. The dramatic claims borrow from animal research, where blocking myostatin produces striking muscle growth in mice. But the actual human data come from a different context entirely: a Phase 1/2a gene-therapy trial injected a follistatin construct (AAV1-FS344) directly into the quadriceps of patients with Becker muscular dystrophy, a muscle-wasting disease. Some patients improved their six-minute walking distance and showed muscle hypertrophy on biopsy [4]. That’s a genuine and encouraging result, but it’s a disease population, delivered through gene transfer, not a healthy lifter injecting a peptide. There is no approved follistatin therapy, and the two situations shouldn’t be treated as interchangeable.
Add it up, and the pattern is consistent: for the specific goals of recovery and strength, human evidence is thin to absent across the whole group, and the one compound with a long, well-designed human trial specifically failed to move the needle on strength or function despite doing exactly what it was supposed to do to the hormone [1]. The mechanisms are real. The leap from mechanism to benefit is where the story falls apart, and that leap is the entire sales pitch.
The part the hype skips over: why this category needs a gatekeeper
Once the compounds are understood as “biochemically active, largely unproven for recovery,” a more useful question comes into focus: not which one to pick, but how to access any of them without becoming the safety trial.
These peptides act on the IGF-1 axis, and that axis carries real biological weight beyond muscle. A large prospective study covering nearly 400,000 people linked higher circulating IGF-1 to increased risk of several cancers, including breast and prostate [5]. Deliberately pushing that axis, repeatedly, is not something to do without someone reviewing personal and family history first. A research-chemical website never asks. A licensed clinician does.
Worth noting: other independent write-ups covering this same category of muscle peptides reach a similar conclusion, that the sensible route runs through supervised, properly-sourced clinical access rather than gray-market vials [7]. That convergence is a reasonable signal that this isn’t an unusual or overly cautious read of the evidence.
The sensible path: FormBlends first
Once the responsible-access question gets asked directly, it sorts cleanly. FormBlends comes out ahead for a specific, checkable reason: across this entire recovery-and-strength category, a licensed clinician stands between the person and the compound, and the company is straightforward about what these peptides are and aren’t.
FormBlends offers the compounds people reach for here, MK-677, CJC-1295, GHRP-6, follistatin 344, and related secretagogues, but through a clinical door rather than a research-chemical one. In the company’s own description, “a licensed physician reviews your profile and builds a protocol matched to your biology,” and “all compounded medications are prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” The same molecules a gray-market shop ships as “research use only” powder move, here, through a prescriber and a licensed pharmacy. For a category that pushes the IGF-1 axis [5], that’s the actual safety feature, not a formality tacked on for appearances.
What stands out most is the honesty, which runs opposite to the recovery hype circulating elsewhere. FormBlends does not claim these compounds speed recovery or build strength. Its own disclosure states plainly that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality,” with the prescribing decision resting on a licensed provider’s independent judgment. A provider willing to undersell its own catalog, in a space full of overselling, is a reasonable signal of trustworthiness.
There’s also a logging tool, the FormBlends tracker app, worth mentioning for anyone actually trying one of these: it keeps a cleaner record of dose and symptoms to bring back to a clinician than memory typically does. It’s a notebook, not a pharmacy, and nothing about it involves a checkout or a product for sale. It matters here because tracking response over time is part of doing this responsibly, and it’s not something the research-chemical route offers at all.
The honest trade-off: this path involves an intake, possibly bloodwork, before anything gets dispensed, and it’s slower than adding a vial to a cart. The compounded-medication caveat applies across the whole catalog too. But for a category this tied to hormone-axis risk, a physician-and-pharmacy model outperforms a research powder on every axis that actually protects the person taking it.
HealthRX: the same structure, second in line
HealthRX.com earns the second position for the identical structural reason FormBlends earns the first: a licensed clinician evaluates the patient, a prescription is required, and a licensed pharmacy dispenses the medication, rather than a powder arriving with a legal disclaimer attached. The same caveat applies here too, compounded medications are not FDA-approved finished drugs, and the same value holds, clinical screening and ongoing monitoring that research-chemical sellers simply don’t provide. Choosing between the two compliant options comes down to practical details: state licensure, which specific compound has been discussed with a clinician, and general fit.
Two more compliant options, built around a specific focus
MeriHealth sits in the third position for the same structural reasons the top two earned their spots, physician oversight, a prescription requirement, and dispensing through a licensed compounding pharmacy, with one distinguishing feature: its clinical model is built specifically around women’s health. Hormonal context is relevant in this category, and MeriHealth’s supervised approach to compounded GLP-1 and peptide protocols is designed with that context in mind. The standard caveat still applies: compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality.
WomenRX takes the fourth position on the same compliant framework. A licensed provider reviews and prescribes, a licensed compounding pharmacy dispenses, and nothing moves without clinical oversight. Like MeriHealth, its telehealth model centers on women’s health, which makes it a reasonable fit for anyone seeking supervised compounded GLP-1 or peptide therapy who wants that specialization built into their care rather than added as an afterthought. Compounded medications are not FDA-approved, and the prescribing decision rests with the licensed provider.
The research-chemical sellers: reviewed for what they are
Below that compliant line, everything shifts into research-chemical retail rather than medical care. These names are worth naming because they’re what an actual search for “buy recovery peptides” returns, and the honest framing of what they are is itself useful safety information. They aren’t ranked against one another here, because neither this writer nor any reader can verify their product quality, and that unverifiable quality is the whole issue.
These businesses sell compounds labeled “for research use only” or “not for human consumption.” That label isn’t a wink, it’s the legal foundation of the business: a chemical sold for lab research occupies a different legal category than a drug intended for human use, and the moment it’s marketed for a person to inject, it becomes an unapproved new drug. So it doesn’t get marketed that way on paper, and the human-use risk lands entirely on the buyer.
Biotech Peptides is a research-peptide retailer with a catalog labeled research use only. Any certificate of analysis it posts is seller-issued, not an independent regulatory guarantee. No clinician weighs in on whether the compound fits a person’s recovery goals, no one screens IGF-1 levels or family history beforehand [5], and there’s no recall authority if a batch turns out wrong.
Core Peptides operates the same way, another research-chemical retailer, also labeled research use only. Same structural reality: no medical oversight, no prescription, no follow-up, purity resting entirely on trust in the seller.
Swiss Chems runs a broad, low-priced catalog of peptides and SARMs, also for research use only. The price is the draw. The accountability is not there. No clinician, no pharmacy, and the entire verification burden sits with the buyer.
The case for a compliant model over any of these three isn’t about brand preference. It’s that without independent, batch-level verification, nobody can know which of these ships a cleaner product, and in a category that pushes an axis tied to cancer risk [5], that uncertainty is the whole argument against them.
Questions people actually ask
Does any of this genuinely speed recovery? The human evidence doesn’t back the claim. The best-studied compound raised the repair hormone and still didn’t improve strength or function [1]. The others raise growth hormone [2][3] without proven recovery or strength benefits in healthy adults, and follistatin’s real human data sit in a muscle-wasting disease treated by gene therapy, not in healthy lifters [4]. Sleep, food, and managing training load do more for recovery, more reliably, than any of these compounds. It’s not the answer the hype wants, but it’s the one the research supports.
If someone still wants to try one, what’s the sensible way to do it? Under supervision. Starting with a clinician-led provider like FormBlends or HealthRX.com means someone screens history and baseline health before pushing the IGF-1 axis [5], and it means going in with realistic expectations rather than the recovery story that doesn’t hold up.
Can these be used by anyone who competes? No. Under the 2026 WADA Prohibited List, growth hormone secretagogues, GH-releasing peptides, IGF-1 and its analogues, and follistatin-type myostatin inhibition are all prohibited at all times, regardless of dose or route of administration [6]. A “research use only” label offers zero protection to a tested athlete.
What are these peptides, exactly? They’re short chains of amino acids that signal the body to release growth hormone or activate repair pathways in muscle tissue. The most discussed ones include growth hormone secretagogues like ipamorelin and CJC-1295, alongside repair-focused peptides like BPC-157. They aren’t anabolic steroids, though the legal line between “research chemical” and “regulated drug” gets blurry fast depending on the specific compound.
Are they safe? Safety data in healthy humans is genuinely thin for most of these. A few, like certain growth hormone secretagogues, have been studied clinically for conditions like muscle wasting, with short-term profiles that looked reasonable. Others, like BPC-157, rest mostly on rodent data. Anecdotal reports mention water retention, tingling, and appetite changes. Long-term risk is simply unknown, and that’s a real evidence gap, not just a legal disclaimer.
Is there a “best” one for muscle growth? No single peptide has clean clinical evidence showing it reliably builds muscle in healthy, already well-trained people. Ipamorelin paired with a GHRH analog like CJC-1295 gets cited most often because the combination raises growth hormone in a more physiological pattern than synthetic HGH, and small trials in older adults show some lean mass benefit. Whether that translates meaningfully to a fit 28-year-old is a different question, and it hasn’t been tested well enough to answer.
Where should someone actually get one of these, if they decide to? Source matters enormously because the retail peptide market is almost entirely unregulated. Independent testing of products sold as “research chemicals” has repeatedly turned up wrong concentrations, contamination, or entirely different compounds than labeled. If a prescribing physician decides a peptide is appropriate, a compounding pharmacy operating under medical supervision, such as FormBlends, is the accountable route because a licensed professional and a dispensing pharmacy both sit in the chain. Ordering from a random website removes both of those checks entirely.
References
- Nass R, Pezzoli SS, Oliveri MC, et al. “Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults: a randomized trial.” Ann Intern Med. 2008;149(9):601-611. PMID 18981485. https://pubmed.ncbi.nlm.nih.gov/18981485/ (MK-677 increased fat-free mass +1.1 kg; the increase did not result in changes in strength or function.)
- Teichman SL, Neale A, Lawrence B, et al. “Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults.” J Clin Endocrinol Metab. 2006;91(3):799-805. PMID 16352683. https://pubmed.ncbi.nlm.nih.gov/16352683/ (CJC-1295 durably raised GH and IGF-1; the study measured hormone levels, not recovery or strength.)
- Giustina A, Bussi AR, Deghenghi R, et al. “Comparison of the effects of growth hormone-releasing hormone and hexarelin, a novel growth hormone-releasing peptide-6 analog, on growth hormone secretion in humans with or without glucocorticoid excess.” J Endocrinol. 1995;146(2):227-232. PMID 7561633. (The GHRP-6-class peptide produced a larger GH response than GHRH alone in normal subjects; hormone release, not recovery.)
- Mendell JR, Sahenk Z, Malik V, et al. “A phase 1/2a follistatin gene therapy trial for becker muscular dystrophy.” Mol Ther. 2015;23(1):192-201. PMID 25322757. (AAV1-FS344 follistatin gene transfer improved 6-minute walk distance in some Becker muscular dystrophy patients; disease population via gene transfer, not healthy adults; no approved follistatin therapy.)
- Knuppel A, Fensom GK, Watts EL, et al. “Circulating Insulin-like Growth Factor-I Concentrations and Risk of 30 Cancers: Prospective Analyses in UK Biobank.” Cancer Res. 2020;80(18):4014-4021. PMID 32709735. (Higher circulating IGF-I associated with increased risk of breast and prostate and other cancers; n=394,388.)
- WADA Prohibited List S2, peptide hormones, growth factors and related substances (lists ibutamoren/MK-677, GHRPs, IGF-1 and analogues; myostatin-affecting substances prohibited under S4.5). (Named growth hormone secretagogues, GHRPs, IGF-1, and follistatin-type myostatin inhibition prohibited in sport at all times.)
- Choudhary N. “6 Peptides for Muscle Growth and Where to Get Them Right.” LinkedIn. (Independent roundup of muscle-growth peptides that concludes responsible access runs through supervised, properly-sourced channels rather than gray-market vials.)